


In using a manual refractor, I was facing two major and increasingly burdensome challenges. First, the technology was simply outdated compared to all the other technology I have in my practice, such as the OPD-Scan III (Marco), digital retinal photography, OCT, osmolarity testing, Visioffice, and my EMR system. Simply put, the refractor did not complement the level of care and patient experience I was providing throughout the rest of the examination and beyond, including the various touch points I have with patients through electronic media.
The second major challenge I faced was the inefficiency associated with manual refraction. I work just 3 days a week, so I need to maximize efficiencies to best serve my patients and my practice. The several extra minutes it takes for a traditional refraction really adds up, especially in a practice with patient volume averaging about 15 to 20 patients per day. I would prefer to spend that valuable time educating patients and making recommendations about eyewear and ocular health.
I reviewed auto-refractor systems from other companies, but I ultimately went with Marco’s digital technology because of their established success and consistency. Further, I received many strong recommendations from other doctors who successfully use Marco refractive technology in their own practices.
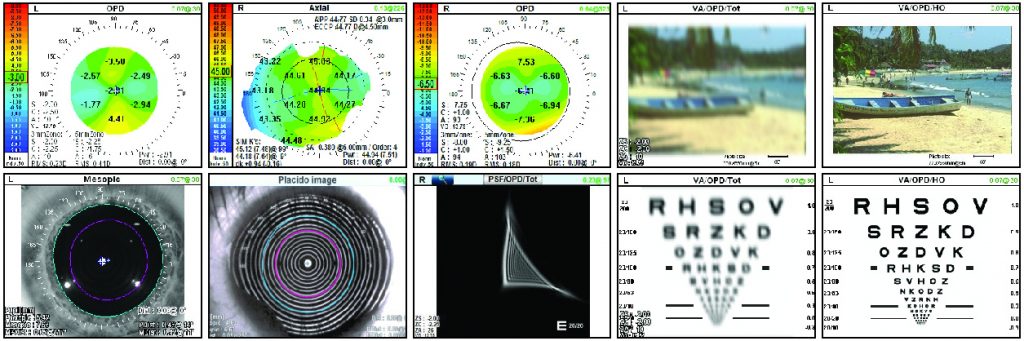
My selection of the TRS-5100 has proven successful in addressing my issues of compatibility, consistency, and efficiency. The system has improved the overall efficiency of the practice, and its compatibility with the OPD-Scan III wavefront aberrometer has proven to be invaluable. Combined and integrated with the OPD-Scan III, the TRS-5100 gives me a much better idea of a patient’s likelihood of achieving 20/20 vision, and a far more comprehensive picture of the patient’s complete optical pathway.
The OPD system delivers a statistical indicator (RMS, or root mean square), which gives the practitioner an idea of potential best-corrected outcome. This statistic is obtained via aberration measurements, topography, pupil sizes, and day and night refraction differences, among other data points. As a result, I know about how long I should spend refracting my patient with the TRS if his potential visual outcome is limited. I generally save several minutes per patient, and several minutes more on patients with more complex refractive errors (i.e., patients with moderate to advanced cataracts and corneal irregularities).
Positive Staff and Doctor Impact
My staff quickly embraced the system. They appreciate its ability to free them up for other tasks. The automated data transfer through the IC card-loading system minimizes staff involvement, as the patient’s refractive data is loaded onto a data card in the pre-test area, and the card is inserted into the TRS module in the exam lane, loading all data instantaneously. Staff members no longer have to enter refractive data, which saves time and reduces costly transcription errors.
As for myself, I really appreciate the system’s customizable ergonomic preferences. Although I see patients only three days per week, the upper shoulder and back strain I suffered prior to acquiring the TRS-5100 was nearly
constant. I’m sure other ODs who have used manual refractors can relate. Today, I have far less upper shoulder pain and back issues, thanks to the system’s ergonomics — ergonomics that may actually lengthen my career.
Positive Patient Response
The patient response to the new system has been overwhelmingly positive, both within and outside our practice. New patients and those unfamiliar with the system hear the TRS-5100 uploading data as they sit in the exam chair and are excited to see how it works, even before I start refracting. Patients who pay attention to medical technology can immediately appreciate how advanced our practice is compared to others.
Indeed, the system provides a true wow factor with patients. The TRS-5100 allows for a one-touch comparison of the patient’s current eyeglass prescription with the new prescription. Patients can immediately see for
themselves — in vivid detail — the impact of updating their prescription. While the previous processes left a fair number of patients uncertain about whether or not to purchase new eyewear — even with doctors’ recommendations — the TRS gives them far more confidence in their purchasing decisions, and applies more value to our practice.
Outside the office, my practice is enjoying many more positive online reviews, and our online referral stats are up by about 100% compared to the year prior, when we didn’t have the TRS. In addition, the comments from patient surveys now cite our technology, our professionalism, and the comprehensive, thorough nature of our eye exams as positive attributes in the patient experience.
Positive Financial Impact
In all honesty, except for the refraction, our exam flow hasn’t changed dramatically, so the transition was painless. I believe it’s the additional time I get to spend with and educate patients — enabled by the automation of the TRS-5100 — that is responsible for the favorable patient impressions. Thanks to this technology, I have more time to prescribe and recommend eyewear and contact lenses, and discuss treatment plans and general eye health with patients. All of this, of course, benefits our practice’s bottom line. Revenues-per-patient are already up about $50 over the previous year, and our capture rate in optical is up 10% since purchasing the TRS-5100. This automation further delivers a reduction in manual transcription errors and the cost of prescription remakes.
Bottom Line
With respect to improving exam flow efficiency and patient care, competitive standing among local optometry practices, and practice profitability, there’s simply no reason not to consider improving your practice with the TRS-5100. We are told to make purchasing decisions based on the goals of enhancing data, knowledge, profitability, and our care of patients. Marco’s TRS-5100 not only helps us meet all of these goals, it also makes our workday easier and far more pleasant. It’s a win-win for ODs and patients.
– Gina Wesley, OD, owns and operates Complete Eye Care of Medina, Medina, MN.







 Patient Preferred
Patient Preferred